Growth
By Deborah Rotenstein, M.D.
For every child, a primary task of childhood is to grow and develop
ultimately into a mature individual. Physical gi’owth begins with
conception. It is influenced by a variety of factors, many of which we
are only beginning to understand. The interaction between genetics and
environment results in a range of possibilities for children’s height,
and the rate at which children attain their genetic potential varies.
Growth rates
The most rapid growth and development take place during the 40 weeks
prior to birth. The fetus, which begins from a single cell, develops
into a group of cells, which become subspecialized. When a sufficient
number of cells have developed, organ systems emerge.
Birth usually occurs when the fetus is 40 weeks old, but some infants
are born earlier or later. So, even at birth, some infants are more
mature physically than others.
After the first 2 years, children begin to assume their individual
growth patterns, and after age 2 or 3, they assume the growth rate that
they will follow until just before puberty. For the first 6 months of
life, children grow at a rate of 7.2 to 8.8 inches (18 to 22
centimeters) per year. By 1 year, they grow at a rate of 4.4 inches (11
centimeters) per year. At 2 to 3 years they gi’ow 2.8 to 3.2 inches (7
to 8 centimeters) per year, and between 4 and 9 they grow 2 to 2.4
inches (5 to 6 centimeters) per year. Growth rates of less than 2 inches
or 5 centimeters per year after age 2 signal the need for medical
assessment. Because absolute heights at any given age may vary, it is
the pattern of growth that needs to be assessed.
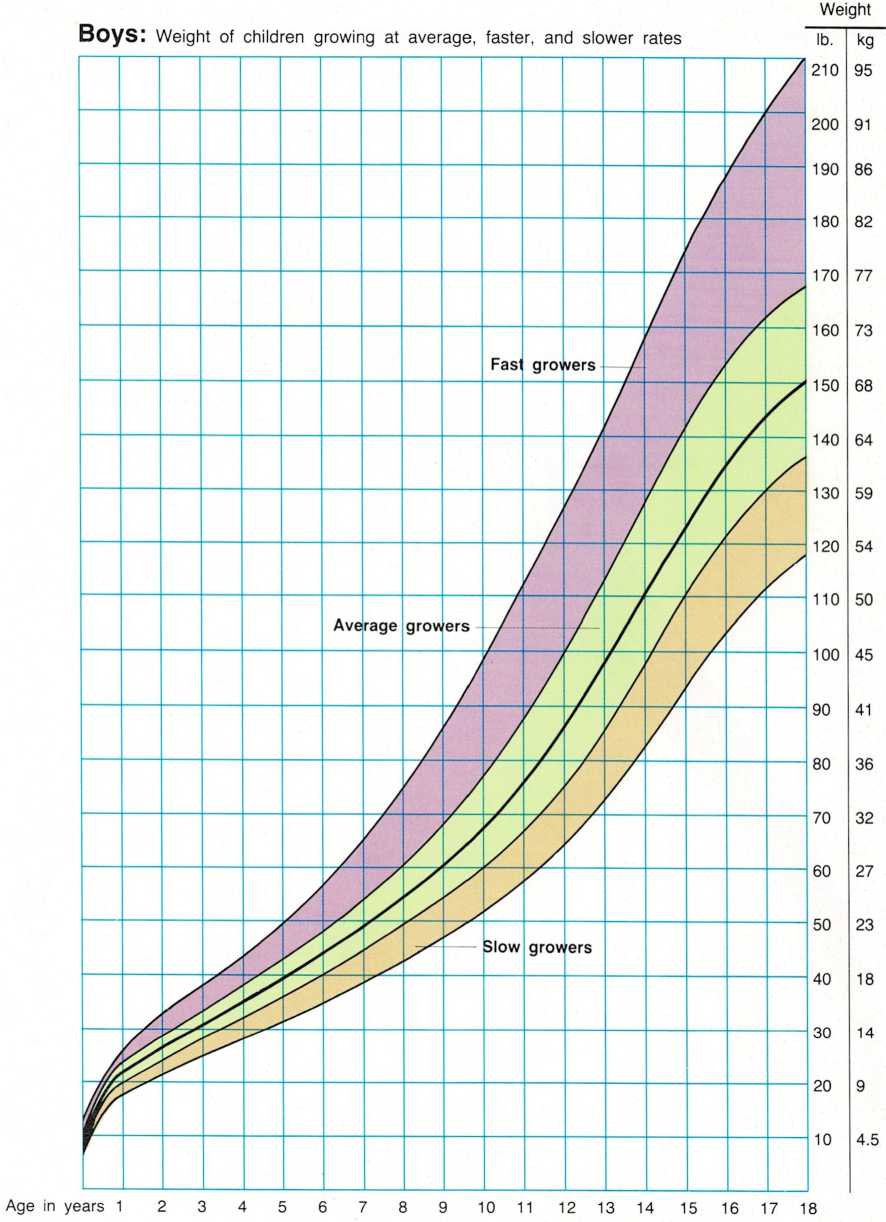
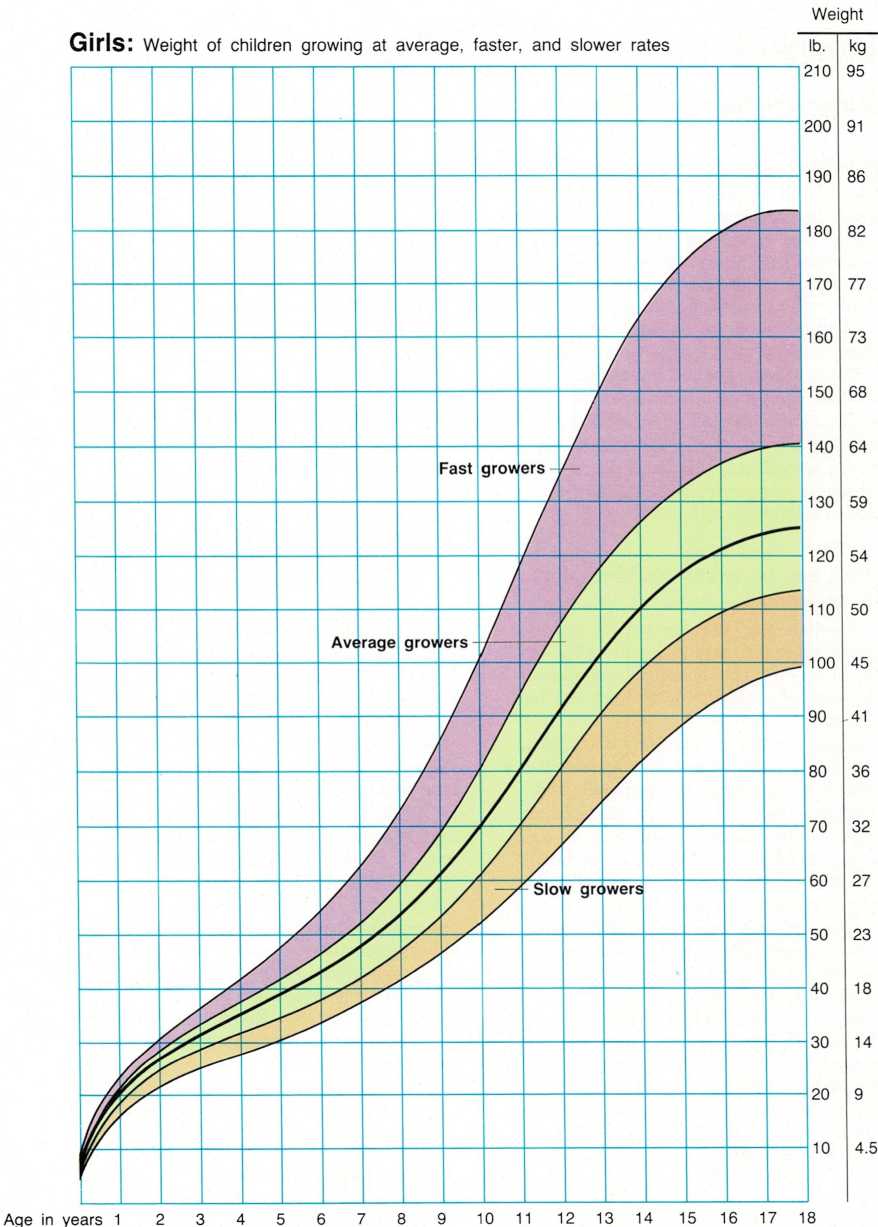
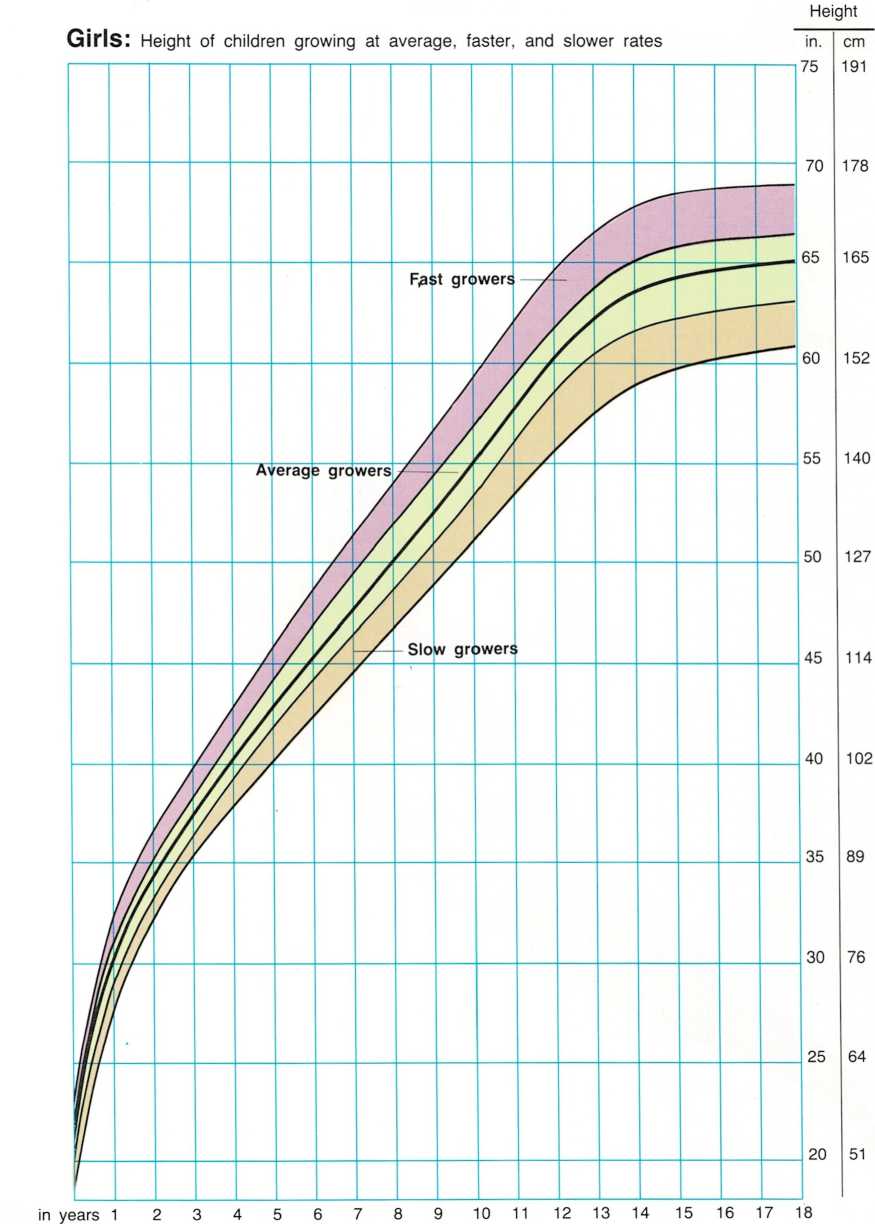
The growth in height and weight for boys and girls at different ages is
shown on the accompanying growth charts. Typical growth in height and
weight is shown by the heavy center line, and faster and slower rates by
the lines above and below it. The variation
in the curves of the lines shows that there are periods of rapid and
slow growth. After the fast growth of the first few years, the changes
become more gradual and then fairly steady. Thin layers of cartilage
called growth plates, found in all long bones, are active throughout
childhood in making the bones grow. There is a spurt of rapid growth
just before growth stops and the growth plates fuse.
The most valuable tool for assessing a child’s growth is a well-kept
growth chart. A child’s height and weight should be measured and
recorded on the growth chart at each visit to the physician. The most
widely used growth charts are made up for boys and girls of all ages and
are divided into ranges of height and weight by per cent. The age in
years is marked along the bottom of the chart, and height (inches and
centimeters) and weight (pounds and kilograms) are marked along the
sides.
Growth differences
Growth patterns of boys and girls differ. In the first 2 years, boys are
slightly taller than girls. After that, until puberty, the heights are
relatively similar. Girls’ skeletal ages—the degree to which their
bones have matured—are generally more advanced at any given age than
are those of boys. Children who are overweight often have a faster rate
of growth and reach puberty earlier than nonobese children.
A child’s rate of growth is not even; it may vary from year to year and
even from season to season, and is often fastest in the spring and
summer. For this reason, growth evaluations should always include
observation for six months to a year.
Short stature
About 3 million children in the United States are shorter than 97 per
cent of their peers. Most of these children are normal in
every way except that they are small. Not all short children have
abnormal growth. However, children who are not growing at an appropriate
rate should be evaluated by their pediatricians.
Some children may be short because they come from a short family, and
the genetic potential for height is small. Other children have a delay
in puberty or a delayed growth spurt, a condition called constitutional
growth delay. These children are shorter than their peers, but
ultimately will reach normal adult height.
World-wide, malnutrition or undernutrition is the most common cause of
short stature. Severe stress or a deprived environment can also cause
shortness. Many systemic illnesses, such as diseases of the heart,
lungs, pancreas (diabetes mellitus), kidneys, and digestive tract, can
cause poor growth, as can endocrine disorders, such as a lack of thyroid
hormone or lack of growth hormone. Growth hormone, which is one of the
hormones involved in the control of growth, can be completely or
partially deficient. Too much cortisol, a stress hormone, can also cause
shortness.
Children may be small for other reasons. Intrauterine growth
retardation— slow growth before birth—is one factor. It may be
caused by infection, or the mother’s use of alcohol, tobacco, or drugs
during pregnancy. Chromosomal abnormalities can cause shortness and
other genetic problems, such as Down’s syndrome or Turner’s syndrome.
Skeletal abnormalities or bone disease can affect the size and shape of
bones.
Occasionally a child is short for reasons that are totally unclear, and
no specific causes can be found. It is not unusual for children who are
under the age of 2 or 3 to cross percentiles in either direction on
their growth curves. However, after age 2 or 3, a fall away from the
growth curve signals that there may be a problem.
Therapy for shortness is directed at correcting the underlying medical
condition. Most children who are deficient in growth hormone can be
treated with gi’owth hormone only by a pediatric endocrinologist.
Children who are short because of delayed puberty, especially boys, can
also benefit from medical intervention. Psychological
support and/or counseling can often be very helpful to the treatment
process.
Tall stature
Just as there are many children who are small, there are about as many
who are taller than 95 per cent of their peers.
Most tall children have tall parents. Tall boys rarely complain about
their size. However, tall girls may feel ill at ease. Children who are
greater than the 95th percentile or who are growing—and continue to
grow— at an abnormally rapid rate should be checked by a physician.
Abnormal height is most often caused by an endocrine disease or a
genetic condition. There are several endocrine causes of abnormal height
and rapid growth. One is growth hormone excess, which may be caused by a
small tumor in the pituitary gland. A more common cause of unusually
fast growth is early puberty. Genetic conditions that cause abnormal
height are rare, and they often include abnormal body proportions.
Emotional factors of growth
Many short children adapt well to their size and may never have
psychological problems, but others do not. Our society places a great
value on height. Short children often face emotional stress from teasing
and may have difficulty coping. In fact, parents of short children
frequently have difficulty accepting a child’s height and treating the
child according to age level.
Teen-age years are often more difficult for the very short or very tall
child. Often problems of short stature are made more difficult by the
lack of sexual development. For short teen-agers, one problem is being
treated as if they are younger than their actual age, and some of them
react by behaving imma- turely. Tall teen-agers may feel conspicuous and
become very self-conscious.
Of course, a child who has a medical problem should be treated. But
children also need to feel loved whether they are short or tall. For
parents and other adults, one of the most important steps in making life
easier, for a short or tall child, is to accept the child’s size.

Age